EMA Regulatory
EMA Q&A on DDC Classification: What Question 1 Really Means
Quick Answer
EMA's Q&A Question 1 establishes the classification framework for drug-device combinations: products where the medicinal action is principal fall under pharmaceutical legislation (linked to MDR Article 1(9)), while products where the device function is principal with an ancillary medicinal substance are regulated as medical devices under MDR Article 1(8). The classification depends on the principal intended action of the combined product and determines the entire regulatory pathway.
Part 1 of a deep-dive series analyzing EMA's Questions and Answers on MDR/IVDR implementation. This series examines each key question in detail-what it says, what it means in practice, and where regulatory teams most often misinterpret the guidance.
It was past eleven when he finally found the paragraph that answered his question. Three hours of reading the same EMA Q&A document, scrolling past sections on labeling and consultation procedures, circling back to the classification guidance that seemed clear on first reading but became less certain with each re-read.
The product sat in the grey zone-a wound care device with a pharmacologically active coating. Was the coating ancillary to the device, or was it the principal mode of action? The EMA's Q&A Question 1 was supposed to answer exactly this kind of question.
And it does-but not in the way most people expect on first reading. Question 1 doesn't give you a simple yes-or-no classification rule. It gives you a framework for analysis, a set of criteria to apply, and a connection to the MDR articles that define which regulatory pathway your product follows.
Understanding what Q1 actually establishes-and where it deliberately leaves room for case-by-case analysis-is the difference between a confident classification rationale and one that unravels during assessment.
What Question 1 Actually Says
Why this matters: Most regulatory professionals have read Q1 at least once. But the document's formal language obscures the practical implications. Breaking down what Q1 establishes-sentence by sentence-reveals the classification logic that EMA expects you to follow.
EMA's Q&A on implementation of MDR and IVDR (currently Revision 5, January 2025) opens its combination product guidance with the foundational classification question: how do you determine which regulatory framework applies to a product that combines drug and device elements?
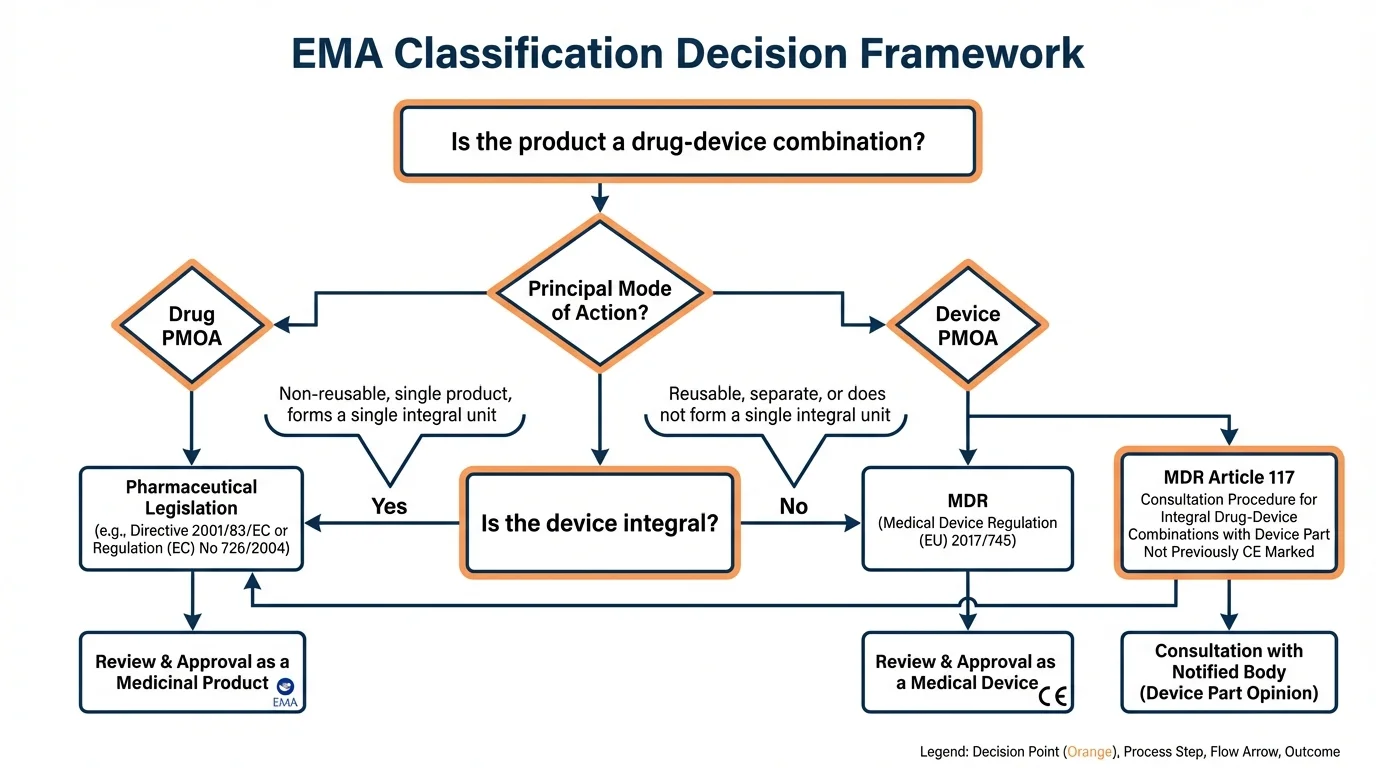
The answer Q1 provides rests on a single principle: the applicable regulatory framework is determined by the principal mode of action of the combined product. This isn't a new concept-it's been the basis of EU combination product regulation since the Medical Devices Directive. But Q1 formalizes how this principle applies under MDR, connecting it specifically to Articles 1(8) and 1(9).
The applicable regulatory framework depends on the principal mode of action of the product. Where the principal intended action is not achieved by pharmacological, immunological, or metabolic means, the product is a medical device which may incorporate a medicinal substance with ancillary action. Where the principal intended action is achieved by such means, the product is a medicinal product.
The key phrase is "principal intended action." Not the most prominent component. Not the most expensive component. Not the component that appears first in the product name. The action that the product is principally intended to achieve-and the mechanism by which it achieves it.
The Classification Framework from Q1
Why this matters: Q1 doesn't just tell you what the law says-it establishes the analytical path that assessors will follow when evaluating your classification rationale. Your documentation needs to mirror this framework.
Q1 Classification Decision Framework
Question
How does the product achieve its principal intended therapeutic effect?
Medical Device under MDR - Article 1(8)
The device function is principal. Medicinal substance supports but doesn't drive the therapeutic effect. Requires NB assessment with medicinal authority consultation on the substance.
Medicinal Product under Pharmaceutical Legislation - Article 1(9)
The medicinal action is principal. Device component is integral but ancillary to drug delivery or function. Requires MA with NB Opinion on device conformity (Article 117).
Seek NCA Formal Classification Advice
When neither action is clearly principal, formal guidance from a national competent authority is recommended before submission. Document your analysis thoroughly.
Separate Regulation Applies to Each Component
The medicinal product and medical device are regulated independently under their respective frameworks. Different from integral DDCs covered by Q1.
Articles 1(8) and 1(9): The Two Categories
Why this matters: These two MDR articles define the legal categories that Q1's classification framework maps onto. Understanding the distinction between them is essential for knowing which requirements apply to your product.
MDR Article 1 establishes the regulation's scope and explicitly addresses combination products. Two subparagraphs define the categories relevant to drug-device combinations:
MDR Article 1(8) vs Article 1(9)
| Aspect | Article 1(8) - Device-Led | Article 1(9) - Drug-Led |
|---|---|---|
| Principal Action | Physical/mechanical (device function) | Pharmacological/immunological/metabolic (drug function) |
| Medicinal Substance Role | Ancillary - supports device function | Principal - device delivers or enables drug action |
| Primary Regulation | MDR 2017/745 (medical device framework) | Directive 2001/83/EC or Regulation 726/2004 (pharmaceutical framework) |
| Assessment Body | Notified Body (with medicinal authority consultation) | EMA or NCA (with Notified Body Opinion per Article 117) |
| Examples | Drug-eluting stent, antimicrobial wound dressing | Pre-filled syringe, autoinjector, on-body delivery system |
| Market Authorization | CE Marking | Marketing Authorization (MA) |
The practical consequence of this distinction is profound. An Article 1(8) product goes through Notified Body conformity assessment as a medical device-with the NB consulting a medicinal authority about the substance. An Article 1(9) product goes through marketing authorization as a medicinal product-with the marketing authorization applicant obtaining a Notified Body Opinion on the device component per Article 117.
Same combined product concept. Completely different regulatory pathway, assessment body, documentation requirements, and timelines-all determined by which mechanism of action Q1's framework identifies as principal.
DDC Types and Their Classification
Why this matters: Abstract classification criteria become clearer through concrete product examples. Knowing how common DDC types are classified under Q1's framework helps you position your own product within the right category.
Drug-Led (Article 1(9) - Medicinal Product Pathway)
- • Pre-filled syringes - Drug is principal; syringe delivers
- • Autoinjectors - Drug is principal; device enables self-administration
- • On-body delivery systems - Drug is principal; patch/pump delivers over time
- • Inhalation devices with drug - Drug is principal; inhaler delivers to lungs
- • Transdermal patches - Drug is principal; patch enables absorption
- • Implants releasing drug - Where drug release is the principal therapeutic action
Device-Led (Article 1(8) - Medical Device Pathway)
- • Drug-eluting stents - Mechanical support is principal; drug prevents restenosis
- • Antimicrobial wound dressings - Physical barrier is principal; antimicrobial is ancillary
- • Bone cements with antibiotics - Structural support is principal; antibiotic prevents infection
- • Heparin-coated catheters - Catheter function is principal; heparin prevents clotting
- • Joint replacement with drug coating - Mechanical function is principal
- • Surgical meshes with antimicrobial - Physical support is principal
Borderline Cases (Require Case-by-Case Analysis)
These products don't have immediately obvious classification under Q1 because both mechanisms contribute meaningfully to the therapeutic effect:
- • Wound gels with growth factors - Is the gel matrix or the growth factor principal?
- • Barrier-forming reflux products - Physical barrier vs chemical neutralization
- • Implants with both structural and pharmacological action - Contribution analysis required
- • Products with evolving scientific understanding - What was once considered physical may now be understood as pharmacological
Classification Evidence Requirements
Why this matters: A classification claim without supporting evidence is an assertion, not a rationale. Q1 implicitly requires manufacturers to substantiate their classification with scientific documentation that an assessor can independently evaluate.
Classification Evidence Checklist (Derived from Q1 Criteria)
- Documented mechanism of action analysis for each active component (drug and device)
- Scientific justification identifying which mechanism achieves the principal intended therapeutic effect
- Clinical data or literature supporting the claimed principal mode of action
- Analysis of comparable products and their regulatory classifications in the EU
- Assessment of whether the medicinal substance action is 'principal' or 'ancillary' relative to device function
- Reference to relevant MDCG guidance documents (particularly MDCG 2022-5 for borderline cases)
- For borderline products: NCA classification advice or EMA ITF input, if obtained
The depth of evidence required scales with classification certainty. A pre-filled syringe delivering an established biologic needs relatively straightforward classification justification-it's clearly drug-led. A novel wound care product with both physical and pharmacological action components requires substantially more analysis and may benefit from formal NCA classification advice before submission.
Common Misinterpretations of Q1
Why this matters: Misunderstanding Q1 leads to incorrect classification rationales that assessors will challenge-potentially invalidating your entire regulatory strategy late in the process.
Misinterpretation 1: "The most valuable component determines classification"
Wrong. Classification is based on principal intended action, not commercial value, manufacturing cost, or which component the company considers primary. A device that costs ten times more than the drug it delivers is still a drug-led combination if the pharmacological action is principal.
Misinterpretation 2: "Q1 provides a definitive classification rule"
Partially wrong. Q1 provides a framework, not a lookup table. For clear cases (pre-filled syringe, drug-eluting stent), the framework yields obvious answers. For borderline products, Q1 deliberately leaves classification to case-by-case analysis-and recommends formal NCA advice for genuinely ambiguous cases.
Misinterpretation 3: "Article 1(8) and 1(9) are the same as integral vs co-packaged"
Wrong. Articles 1(8) and 1(9) both address integral combinations-they differ in which action (device or drug) is principal. Co-packaged products, where the drug and device are not physically integrated, fall outside the Q1 classification framework and are regulated separately under their respective frameworks.
Misinterpretation 4: "Our US PMOA determination applies in the EU"
Wrong. While the underlying concept is similar, an FDA PMOA determination has no regulatory standing in the EU. EU classification must be independently justified under the MDR framework and Q1's criteria. The analysis may reach the same conclusion, but it must be documented separately using EU regulatory references.
Applying Q1 to Your Product
Why this matters: Knowing what Q1 says is necessary; knowing how to apply it to your specific product is what prevents classification challenges during assessment.
Step 1: Map the Mechanisms
Document every mechanism by which your product achieves its therapeutic effect. For each mechanism, categorize it as pharmacological, immunological, metabolic, or physical/mechanical. Be exhaustive-assessors will look for mechanisms you haven't addressed.
Step 2: Identify the Principal Action
Ask: which mechanism makes the most important contribution to the overall intended therapeutic effect? This isn't about which component is larger, more expensive, or more complex-it's about which action the product is principally intended to achieve.
Step 3: Map to Article 1(8) or 1(9)
If the principal action is physical/mechanical with an ancillary medicinal substance → Article 1(8) → device pathway. If the principal action is pharmacological/immunological/metabolic → Article 1(9) → pharmaceutical pathway. If genuinely unclear → proceed to Step 4.
Step 4: Seek Guidance (If Needed)
For borderline products, consult MDCG 2022-5 guidance and consider requesting formal NCA classification advice or EMA Innovative Task Force input. Document the consultation and its outcome as part of your classification rationale. PMOA determination guidance provides the detailed analytical framework.
References
- 1. EMA Questions and Answers on implementation of MDR and IVDR (EMA/37991/2019 Rev.5, January 2025), Question 1
- 2. Regulation (EU) 2017/745 (MDR), Articles 1(8) and 1(9) - Scope for combination products
- 3. Directive 2001/83/EC - Medicinal products for human use, as amended by MDR Article 117
- 4. MDCG 2022-5 - Guidance on borderline between medical devices and medicinal products under MDR
- 5. Regulation (EC) No 726/2004 - Centralized procedure for medicinal products
Need faster answers? RegulatorySense delivers instant, authoritative guidance with source citations.
FAQ
What does EMA's Q&A Question 1 address regarding drug-device combinations?
What is the difference between MDR Article 1(8) and Article 1(9)?
How does Q1 relate to PMOA determination?
What evidence does EMA expect to support classification under Q1?
Does Your Classification Hold Up to EMA's Criteria?
EMA's Q1 sets the framework. Your classification rationale either meets it or doesn't. Two minutes to verify your reasoning against the criteria that matter.
Stop searching through hundreds of PDFs. Get authoritative answers in seconds.
Verify Your Classification →5 questions · Personalized insights · Free